<< Back to online CE course catalog
The Romberg sign has long served as a foundational component of the neurological examination in chiropractic practice, offering a clinical window into proprioceptive integrity, posterior column function, and the sensory contributions to postural control. While its use has been widespread for more than a century, the scientific community has subjected this procedure to increasing critical scrutiny — raising questions about its diagnostic accuracy, its ability to differentiate vestibular from somatosensory dysfunction, and its practical clinical utility. This online chiropractic CE course examines the Romberg sign through the lens of current evidence, helping practitioners make informed decisions about when and how to apply this assessment in today's clinical environment.
Course #209 | 2 CE Hours | $40.00 | Online | PACE & Board Approved
Register for This CourseNamed after the German neurologist Moritz Romberg, this sign was first described in the nineteenth century as a means of identifying the sensory ataxia associated with tabes dorsalis — severe posterior column damage that impairs proprioceptive function. The test's elegance lies in its simplicity: a patient who maintains balance with eyes open but loses it upon eye closure is demonstrating reliance on vision to compensate for deficient proprioceptive input from the dorsal column-medial lemniscus pathway. For decades, this principle made the Romberg sign a standard fixture of the chiropractic and neurological physical examination.
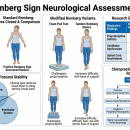
Traditional teachings positioned the Romberg sign as a reliable screen for posterior column and proprioceptive dysfunction, clearly distinguishable from cerebellar disease on the basis that cerebellar dysfunction produces imbalance even with eyes open. However, recent quantitative posturographic research has challenged this clean distinction. Studies demonstrate that the classical Romberg test shows only modest diagnostic discrimination between patients with sensory neuropathy and healthy controls, particularly because elevated body sway under eyes-open conditions in patients with neurological involvement tends to diminish the contrast that the test relies upon. Researchers have further noted that the test does not reliably differentiate vestibular from somatosensory ataxia using conventional administration.
In response to these limitations, modified versions of the Romberg test — including the sharpened tandem-stance Romberg, the foam-pad vestibular Romberg, and single-limb variations — have been proposed to increase sensitivity and improve diagnostic specificity. Emerging evidence supports a refined vestibular Romberg quotient, comparing foam-standing to firm-surface standing under eyes-closed conditions, as a more reliable tool for distinguishing vestibular from somatosensory imbalance. This course helps chiropractors critically evaluate these findings and determine whether and how the Romberg sign should remain part of their clinical toolkit.
Dr. Michael Hall, DC, FIACN is a Fellow of the International Academy of Chiropractic Neurology, a Diplomate of the American Board of Chiropractic Neurology (1993), and a graduate of Parker College of Chiropractic with Honors (1990). He is the founder of BrainDC.org and brings more than 30 years of clinical practice experience to his role as Lead Neurology and Orthopedics Faculty at CCEDseminars. Learn more about Dr. Hall and the full CE faculty team at CCEDseminars Faculty.
What is the Romberg sign and why is it used in chiropractic practice?
The Romberg sign is a clinical test that evaluates proprioception and posterior column integrity by observing a patient's ability to maintain balance with eyes closed. In chiropractic practice, it has traditionally been used as part of a standard neurological assessment to screen for dorsal column dysfunction, sensory ataxia, and conditions affecting the vestibular or proprioceptive pathways.
Is the Romberg sign still considered reliable based on current research?
Recent quantitative research has raised questions about the classical Romberg test's diagnostic discrimination, particularly its ability to distinguish patients with sensory neuropathy from healthy controls or to differentiate vestibular from somatosensory ataxia. The evidence supports interpreting the Romberg sign within the broader context of the neurological examination rather than as a stand-alone diagnostic tool, and highlights that modified Romberg variants may offer improved clinical utility.
How many CE hours is Orthopedics 209 and is it approved for my state license?
Orthopedics 209: The Romberg Sign is a 2-hour online chiropractic CE course that is PACE-approved and accepted by most state chiropractic licensing boards. CCEDseminars maintains approval with numerous boards across the United States. For state-specific acceptance details, review the course guidelines page before registering.
Orthopedics 209 may be applied toward CCEDseminars' structured chiropractic certification and diplomate preparation pathways — explore the full range of options at CCEDseminars Certification Programs.
Chiropractic CE requirements vary by state — verify your board's specific hour requirements and approved course categories before completing your registration at CCEDseminars State CE Guidelines.
Watch Free Chiropractic CE Previews on YouTube
Subscribe to the CCEDseminars channel for course previews, clinical pearls, and CE updates.
Subscribe on YouTubeAlaska, Colorado, Connecticut, Delaware, District Of Columbia, Idaho, Illinois, Indiana, Iowa, Kansas, Maine, Maryland, Massachusetts, Michigan, Minnesota, Missouri, Montana, Nebraska, New Hampshire, New Jersey, New York, North Carolina, North Dakota, Ohio, Oregon, Puerto Rico, Rhode Island, South Carolina, South Dakota, Tennessee, Texas, Utah, Vermont, Virginia, Washington, West Virginia, Wyoming,
British Columbia, Manitoba, New Brunswick, Nova Scotia, Ontario, Yukon,
Argentina, Australia, Bahamas, Belgium, Bolivia, Cayman Islands, Chili, Columbia, Costa Rica, Cyprus, Denmark, Dominican Republic, Ecuador, Fiji, Finland, Greece, Guam, Hong Kong, Hungary, Iceland, Iran, Israel, Italy, Jamaica, Japan, Jordan, Korea, Lebanon, Libya, Liechtenstein, Malaysia, Mexico, Nambia, New Zealand, Northern Ireland, Norway, Panama, Peru, Philippines, Saint Kitts & Nevis, Saudi Arabia, Singapore, Spain, Sweden, Switzerland, Taiwan, Thailand, Trinidad & Tobago, United Arab Emirates, United Kingdom, Venezuela, Virgin Island, Zimbabwe,
 Login
Login